
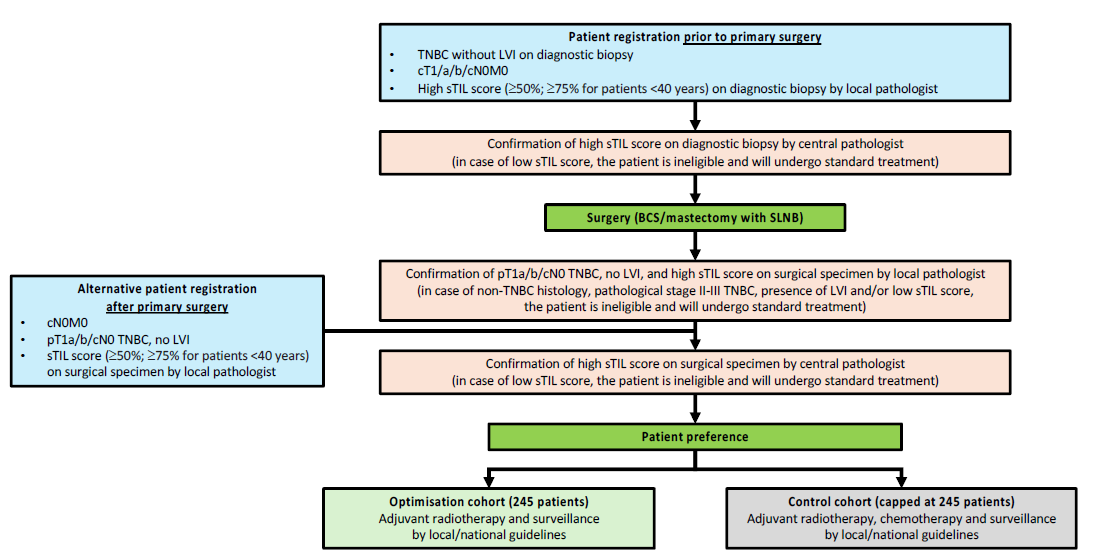
 This study is an international, open-label, pragmatic, patient-preference trial for patients with stage I triple-negative breast cancer (TNBC) and a high sTIL (stromal tumor-infiltrating lymphocytes) score (defined as ≥50% for patients ≥40 years; ≥75% for patients <40 years) to evaluate whether adjuvant chemotherapy can be safely omitted.
This study is an international, open-label, pragmatic, patient-preference trial for patients with stage I triple-negative breast cancer (TNBC) and a high sTIL (stromal tumor-infiltrating lymphocytes) score (defined as ≥50% for patients ≥40 years; ≥75% for patients <40 years) to evaluate whether adjuvant chemotherapy can be safely omitted.